Oncology Optimized Limited Distribution
The NCODA-preferred model for oncology care delivery, Oncology Optimized Limited Distribution, excludes PBM-affiliated mail-order pharmacies while allowing MIPs and non-PBM mail-order pharmacies to dispense. This approach promotes coordinated, in-practice care and ensures timely, person-centered treatment. NCODA remains dedicated to ongoing education and advocacy to expand access to this model wherever possible.

NCODA is committed to collaborating with all stakeholders to demonstrate that the medically integrated pharmacy (MIP) model is the optimal approach for delivering high-quality patient care. While we strive for success across the healthcare ecosystem, our top priority remains achieving the best possible outcomes for patients. Learn more below about MIP and the pillars that drive positive patient outcomes.
NCODA Distribution Model Definitions
Applies to medications with highly restricted networks, such as those requiring REMS or manufacturer-designated controls. These models typically offer little to no flexibility in dispensing, often excluding MIPs altogether. This includes models with no MIP Access.
Represents the NCODA preferred model, where PBM affiliated mail order pharmacies are excluded, and MIPs and non-PBM affiliated pharmacies can dispense. This model enables coordinated, in-practice care and supports timely, patient-centered treatment. NCODA is committed to continued education and advocacy to expand access to this approach wherever possible.
Includes one or two PBM-affiliated mail order pharmacies which include Optum, CVS Caremark, or Express Scripts. While not preferred, it is important to recognize manufacturers that are attempting to promote MIPs and limit access to PBM owned pharmacies.
*This distribution networks limit MIP involvement and introduce barriers to timely access and coordinated care, often through restrictive contracting or payer-driven steerage.
Medications widely available through retail, hospital and mail order pharmacies without restrictions. Includes Optum, CVS Caremark, and Express Scripts PBM-affiliated mail order pharmacies.
*These distribution networks limit MIP involvement and introduce barriers to timely access and coordinated care, often through restrictive contracting or payer-driven steerage.

Redefining Oncology Distribution: Advancing Medically Integrated, Patient Centered Care Through Oncology Optimized Limited Distribution
The number of available oral anti-cancer medications has steadily increased over the past two decades, with oral medications playing a major role in the treatment of multiple tumor types.1 Alongside this evolution, the medically integrated dispensing pharmacy (MIP) has become a best-in-class model for dispensing anti–cancer therapies while preserving a high standard of coordinated, patient centered care.

Experience of physicians, pharmacists, and pharm techs prescribing and dispensing OAMs with a Limited Drug Network within MIPs in the Athena Oncology Network
This white paper presents findings from a targeted survey conducted across the Athena Oncology Network, featuring perspectives from 15 physicians, 15 pharmacists, and 5 pharmacy technicians. Participants shared their experiences with Medication In-Office Dispensing Programs (MIPs), their views on Limited Dispensing Network (LDN) models, and the impact these models have on patient care.
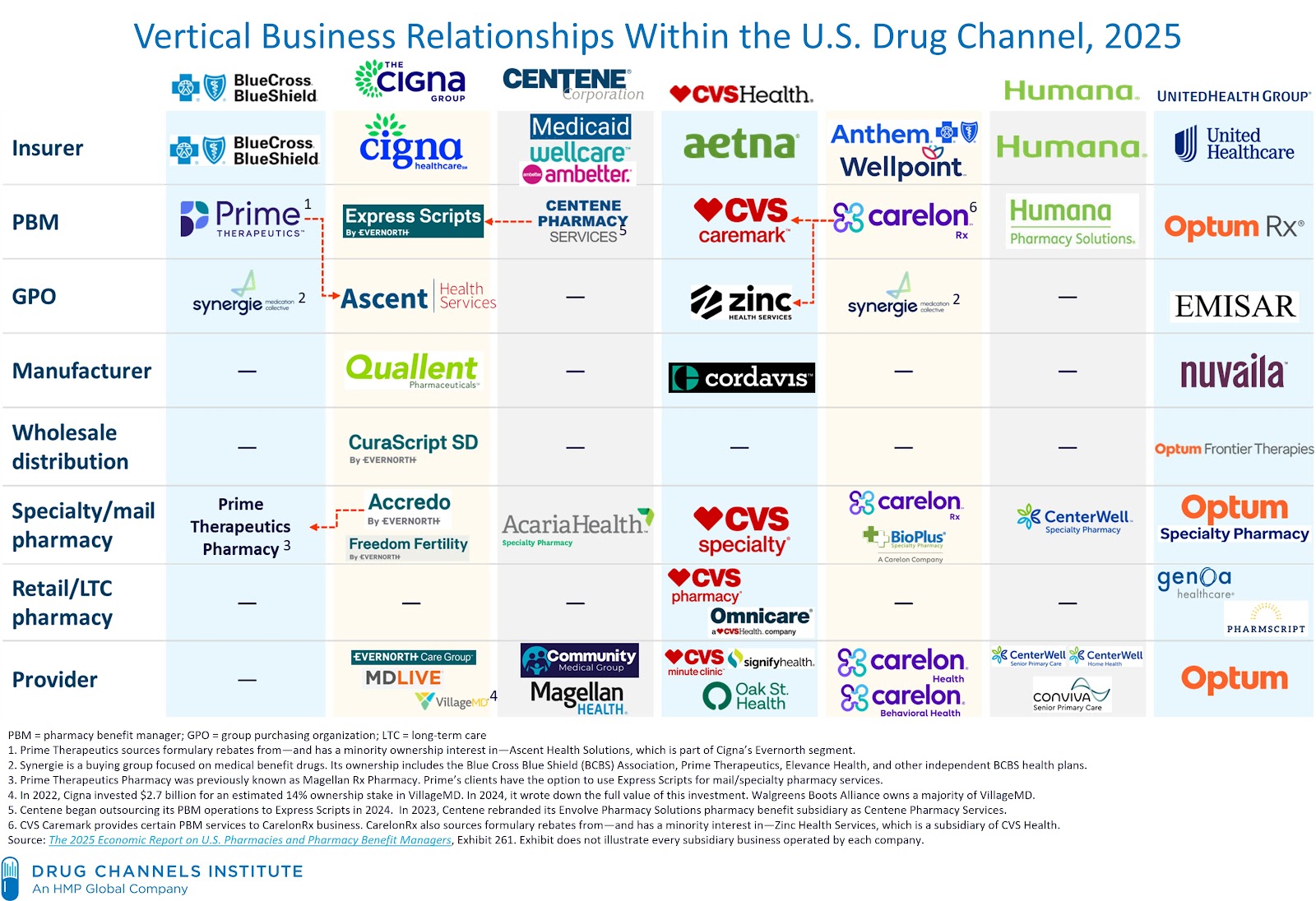
The graphic below highlights the increasing vertical integration across healthcare stakeholders—including insurers, pharmacy benefit managers, specialty pharmacies, and providers. NCODA’s efforts to define limited distribution is grounded in this evolving healthcare landscape. As vertical integration reshapes access pathways, it is critical to understand how LDNs operate within these consolidated structures and the downstream effects on oncology practices and patient care.
Image Provided By: Drug Channels Institute, an HMP Global company